Dedifferentiated Liposarcoma
What is Dedifferentiated Liposarcoma? A high-grade, non-lipogenic sarcoma known as dedifferentiated liposarcoma (DDL) can develop from a well-differentiated liposarcoma. (WDL). It was first reported by the American pathologist Harry L Evans in 1979. The phenomenon of dedifferentiation is time-dependent and up to 90% of DDL cases arise de novo. In the remaining… Read More
Top Doctors For Dedifferentiated Liposarcoma Treatments
















































Top Hospitals For Dedifferentiated Liposarcoma Treatments










































Dedifferentiated Liposarcoma
What is Dedifferentiated Liposarcoma?
A high-grade, non-lipogenic sarcoma known as dedifferentiated liposarcoma (DDL) can develop from a well-differentiated liposarcoma. (WDL). It was first reported by the American pathologist Harry L Evans in 1979. The phenomenon of dedifferentiation is time-dependent and up to 90% of DDL cases arise de novo. In the remaining 10% of cases, DDL develops as a dedifferentiated recurrence of a previous WDL. Unlike WDL, DDL is a high-grade and aggressive disease.
{kind=link}
What are the Predisposing Factors to Dedifferentiated Liposarcoma?
DDL presents most frequently in middle-aged and older adults (more common in people between the ages of 60-70). Men are slightly more likely than women to have the disorder.
Sites of Occurrence
Dedifferentiated liposarcoma is the most frequent retroperitoneal sarcoma. DDL can also occur in the extremities (hands and legs), spermatic cord, and trunk (including mediastinum and thorax). Occurrence in the head, neck, and superficial soft tissue is extremely rare.
Symptoms of a Dedifferentiated Liposarcoma
The symptoms of a dedifferentiated liposarcoma are dependent on its size and location. In the retroperitoneal region, it could lead to abdominal discomfort or pain, early satiety during meals, abdominal mass, weight loss, blood in the feces, constipation, etc. In the extremities, it can lead to swelling of the affected limb, varicose vein, paraesthesia, etc.
How to Diagnose Dedifferentiated Liposarcoma
DDL typically manifests as a sizable, painless mass that has grown slowly over several years. It is usually an incidental find in the retroperitoneum unless clinical signs have been observed. It is the first tumor to consider in a high-grade sarcoma of the retroperitoneum in an adult. The tests conducted if a dedifferentiated liposarcoma is suspected are:
- Complete blood count (CBC)
- Serum chemistry test: this can be used to determine the liver and kidney. This helps in deciding further tests to conduct and the best treatment approach.
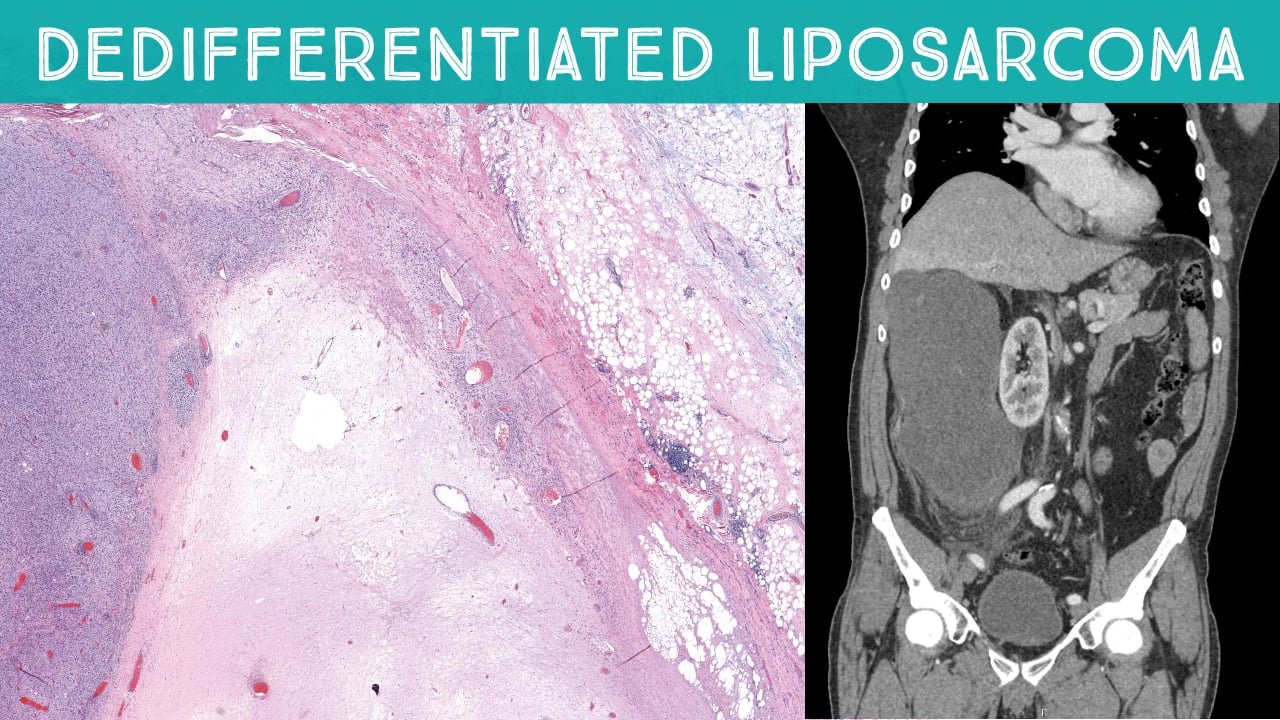
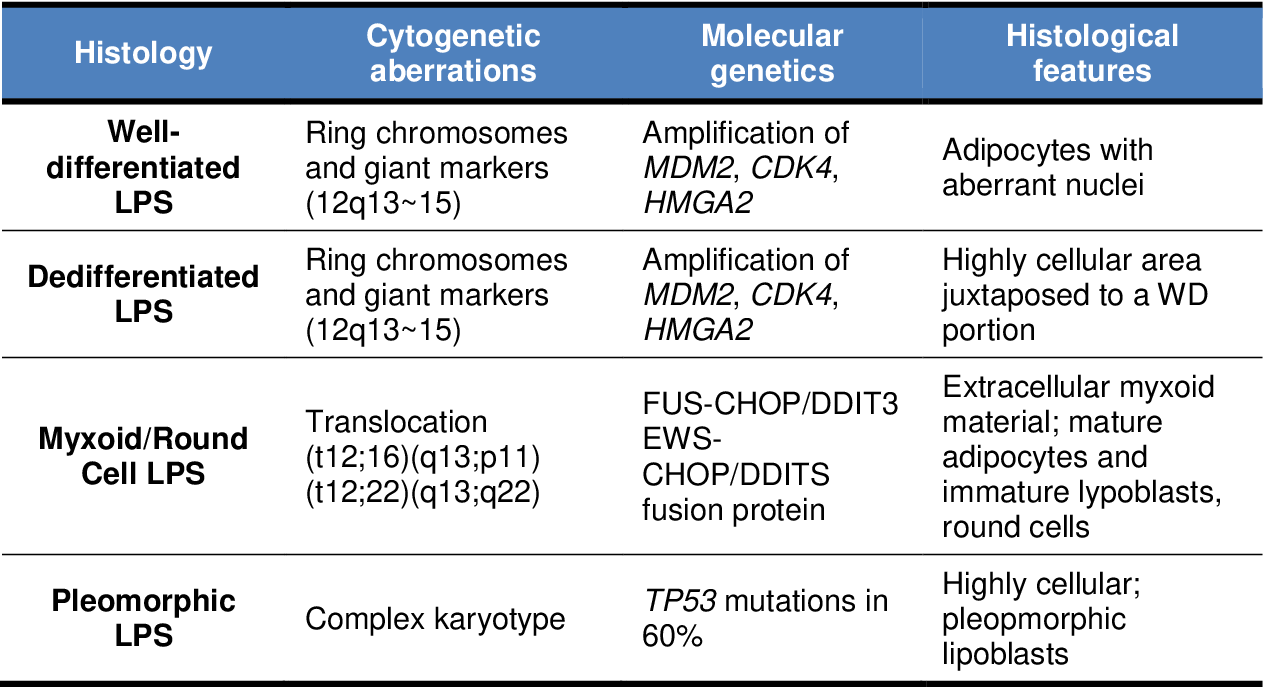
- Biopsy: Samples of the tumor would be collected and examined histologically. Large multinodular tumors with solid, non-fatty, tannish-colored regions and lipomatous yellow areas with gradual or abrupt transition zones are typically macroscopically dedifferentiated liposarcomas. Dedifferentiated liposarcomas have irregular fibroblastic spindle cells with minor nuclear atypia, a varied histological appearance, and sudden or gradual transition zones. (low-grade). Immunohistochemistry stains are usually positive for MDM2 and CDK4 1.
- Ultrasound: DDL usually appears as multilobulated with areas of low echogenicity
- X-rays: X-rays are used to check the kidneys and other organs for possible metastasis. A common radiological feature of dedifferentiated liposarcomas is the coexistence of lipomatous and solid non-fatty components, multinodular tumor margins, and possible displacement of other organs or tissue.
- Computed tomography (CT) scan: This is a better way to look for the presence of tumors in the organs. Typically, a fat tissue density mass with thick or nodular enhancing areas can be seen on a CT scan. Calcifications might be found.
- Magnetic resonance imaging (MRI): This is particularly helpful in determining the presence of cancer and possible metastasis. Dedifferentiated liposarcomas will appear as a mass with juxtaposed fatty and non-fatty components on MRI. The non-fatty components appear heterogeneous with contrast enhancement.
Differential Diagnosis
The common differentials for dedifferentiated liposarcoma include the following:
- Leiomyosarcoma
- Malignant peripheral nerve sheath tumor (MPNST)
- Melanoma
- Pleomorphic liposarcoma (PLS)
- Rhabdomyosarcoma
- Sarcomatoid carcinoma
- Sarcomatoid mesothelioma
- Malignant fibrous histiocytoma (MFH) and undifferentiated pleomorphic sarcoma (UPS)
- Intramuscular lipoma
- Atypical lipomatous tumors/well-differentiated liposarcomas
- Myxoid liposarcoma
- Pleomorphic liposarcoma
- Myolipoma of soft tissue
- Angiomyolipoma
- Teratoma
Treatment of Dedifferentiated Liposarcoma
The treatment or management to be instituted in cases of DDL is dependent on the location of the tumor and if it has metastasized. The treatment regimen may include:
Surgery:
Wide resection is the standard treatment for local disease. If the DDL is in the extremities, this is simple to accomplish. However, retroperitoneal tumors provide more of a challenge. In surgical practice, the selection of which procedure is suitable for an individual patient must be based on tumor location, size, stage, relationship with surrounding neurovascular and bone elements, and functional and cosmetic requirements. The procedures available include:
- Laparoscopic surgery: This involves the use of laparoscopy and surgical tools adapted for the procedure. Small incisions are around the region closest to the site of the tumor. A camera is attached to the laparoscope and passed through the incision the surgical tools are passed through another incision through which the excision is performed. It is best for smaller tumors, although larger tumors can be cut into smaller bits.
- Open surgery: This is done by making a larger incision line. It is used for larger tumors. Unlike laparoscopic surgery, it has a higher risk of postoperative complications, and wound healing takes a longer time.
Non-surgical management:
The development of unresectable local and/or metastatic DDL is associated with a poor prognosis. Different therapies have been adapted to be used in the management either alone or in combination with surgery depending on the patient’s needs. These treatments are:
- Radiotherapy: This involves the use of radiation in the management of cancer. The high-energy protons or x-rays are used to destroy the cancer cells.
- Anthracycline-Based Therapy: Anthracycline-based therapy is a standard first-line treatment for advanced DDL. This involves the use of drugs such as doxorubicin in patients. This drug is very effective in the management of metastatic soft tissue sarcoma.
- Tyrosine Kinase Inhibitors (TKI): Pazopanib is an oral multi-target TKI with anti-angiogenic and antitumorigenic properties and has been approved in multiple countries as a second or later-line treatment for patients with advanced soft tissue sarcoma (STS). Other multi-target TKIs such as sunitinib, regorafenib, and anlotinib have been assessed via clinical trials but are yet to be approved for use.
- Non-taxane microtubule dynamics inhibitor: Eribulin, a non-taxane microtubule dynamics inhibitor, is currently licensed for use in patients with unresectable or metastatic liposarcoma in patients treated with an anthracycline-based regimen in the past.
- Alkylating agents: Trabectedin, a marine-derived drug that binds to the N2 of guanine in the minor groove of DNA, has also been approved for the treatment of patients with unresectable or metastatic liposarcoma in patients treated with an anthracycline-based regimen in the past.
- MDM2-Thargeted Therapy e.g. milademetan and idasanutlin
- CDK4-Thageted Therapy e.g. palbociclib, ribociclib and abemaciclib
- Exportin 1 (XPO1) Inhibitor e.g. Selinexor
Although patients with an advanced form of DDL have a poor prognosis, supportive therapy and care are crucial components of cancer treatment.