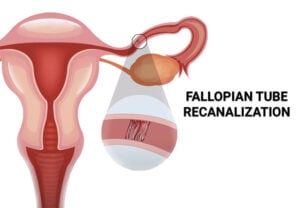
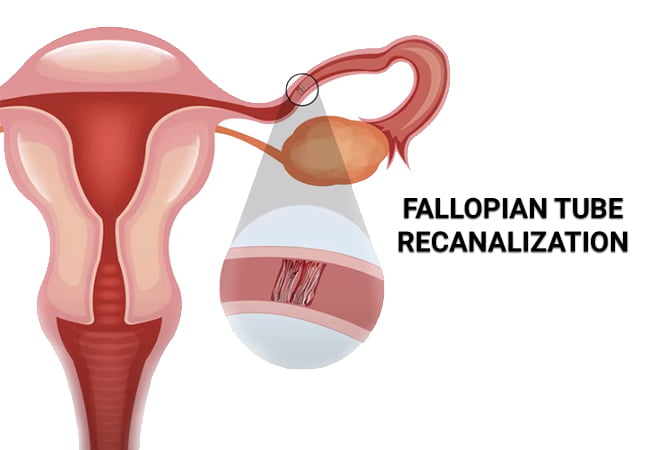
Fallopian Tube Recanalization
The major indications of fallopian tube recanalization are blockages in the proximal and middle portions of the fallopian tube. Fallopian tube recanalization is contraindicated in the following: Read More
Top Doctors For Fallopian Tube Recanalization Treatments






































































































Top Hospitals For Fallopian Tube Recanalization Treatments











































Fallopian Tube Recanalization
What is Fallopian Tube Recanalization?
Fallopian tube recanalization (FTR) is a non-surgical procedure performed to clear blockages of the fallopian tube. Platia and Krudy first described the transvaginal fluoroscopically guided recanalization of the fallopian tube in 1985.
{kind=link}
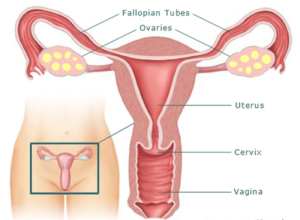
Affectations of the fallopian tube account for the most common cause of female infertility. Conditions like endometriosis and pelvic inflammatory disease can lead to adhesion or occlusion of the fallopian tube. A less common cause of proximal tubal occlusion is salpingitis isthmica nodosa. In a proximal blockage of the fallopian tubes, there is usually the presence of debris which forms a plug in the proximal tube. In a distal blockage, there is hydrosalpinx with dilatation of the fallopian tube mainly due to a previous infection.
{kind=link}
Diagnosis of tubal adhesion or occlusion
A Hysterosalpingography (HSG) is used in the evaluation of fallopian tube patency. It is performed under fluoroscopic guidance during the follicular phase of the menstrual cycle after the cessation of menses. The major side effects or complications of the procedure include infections, pain, and hypersensitivity to contrast medium.
A selective salpingogram with Fallopian tube recanalization (SS-FTR) is a more modern form of the HSG and allows for a precise evaluation of the fallopian tubes.
Indications and Contraindications
The major indications of fallopian tube recanalization are blockages in the proximal and middle portions of the fallopian tube.
Fallopian tube recanalization is contraindicated in the following:
- Genital tuberculosis: Performing a recanalization can lead to a flare-up of subclinical infections.
- Distal tubal occlusions: Due to the location of the occlusion, it is not amenable to catheterization.
- Florid infections: As in genital tuberculosis, recanalization can lead to a flare-up of the infection.
- Obliterative fibrosis: The severity of the fibrosis makes it more likely for the procedure to fail or for a perforation to occur.
- Salpingitis isthmica nodosa: The inflammation of the fallopian tube increases the likelihood of the procedure failing.
- Extensive scarring of the fallopian tubes: As with fibrosis the procedure is not effective in the removal of scar tissues.
- Long tubal obliterations: The nature of the obstruction makes it an unsuitable procedure for the restoration of the patency of the fallopian tube.
Techniques for fallopian tube recanalization
The major techniques used in the correction of proximal and median fallopian tube occlusions are ultrasound-guided, endoscopic, hysteroscopic, and open or laparoscopic surgical approaches. A combination of more than one method may be employed for better results. However, the physician’s preference and technical knowledge also play a role. All these techniques are used in guiding the balloon or wire catheter used in the tuboplasty.
The ultrasound-guided method can be used to guide transcervical recanalization using balloon tuboplasty or catheterization with wire tuboplasty using laparoscopic control. Catheterization can also be guided by ultrasound with the use of an ultrasound contrast agent.
The development of an endoscopic fiber catheter that can be placed transcervical and used to visualize the lumen of the fallopian tube has also been documented. This fiber catheter is used to displace debris that may block the tube, break down intraluminal adhesions and eliminate proximal endoluminal This system consists of a hysteroscope, a flexible coaxial catheter, a guidewire, and a falloposcope with enhanced fiber optics.
Another innovation that allows for the transcervical viewing of the entire tubal mucosa is the use of a linear everting catheter (LEC) in conjunction with a microendoscope. Evaluation of the tubal lumen, tubal wall, and mucosa can be done using this technique while avoiding the need for hysteroscopic guidance and so may be performed with just moderate sedation.
A surgical approach has been described for the recanalization of the fallopian tube and involves the implantation of the most proximal fallopian tube into the uterus. Microsurgical anastomosis, non-cornual implantation, or cornual implantation could all be used to achieve this. It could be done through an open or closed technique. The anatomy of the Utero-tubal junction makes the transcervical procedure preferable.
Procedure
Prior to the procedure, a thorough physical examination is performed. Routine laboratory work is also done. In some instances, perioperative antibiotics are prescribed. The procedure lasts about half an hour. Due to the nature of the procedure anesthetic agents may not be necessary, only analgesics.
- A speculum is placed into the vagina, and the catheter is passed through the cervix into the uterus.
- An iodine-based contrast agent is injected through the catheter, and the uterine cavity is then examined with the help of an X-ray.
- Following this, the image is examined to determine the presence or absence of a blockage and its location.
- In order to remove the obstruction, a smaller catheter is then inserted through the larger one into the fallopian canal.
After the procedure, the patient is observed and discharged.
Complications and risks associated with Fallopian Tube Recanalization
- Spotting: This is a very common side effect of a fallopian tube recanalization but usually resolves within 24 to 48 hours post-surgery. Pads are usually recommended during this period.
- Infections: Secondary bacterial infections may occur if the procedure is not performed under sterile conditions. Signs of a postoperative infection may include fever, vaginal discharge, pelvic pain, etc.
- Fallopian tube perforation: There is a risk of tubal perforation either during the injection of the contrast media or the recanalization process. It is necessary to check for leaks during the HSG. It may also occur in cases of fibrotic tubal obstructions.
- Hypersensitivity reactions: Idiosyncratic reactions to the contrast media have been reported. Some patients are sensitive to the dye, and thus, precautions should be taken during the procedure, and signs of a reaction observed.
- Ectopic pregnancy: Ectopic pregnancies occur in about 3% of women who have undergone a fallopian tube recanalization.
- Peritonitis: This can happen as a result of the spillage of the contrast media into the peritoneum.
- Pain: This is usually uncommon but may occur as a sequela to other complications.
Conclusion
The success rate of Fallopian tube recanalization is as high as 92% and as low as 72%. This makes it a suitable procedure for women with infertility of proximal tubal origins. It is minimally invasive and well-established in the management of infertility. Re-occlusion of the fallopian tube may occur, and thus, a recanalization should be performed.