Abdominal Hysterectomy
Abdominal hysterectomy is performed in an aseptic environment and may be done under general or spinal anesthesia. The surgical incision is made either in a midline or low transverse pattern. Blood vessels are clamped and ligated and depending on the type of necessary tissues cut. The surgical incision is then closed. Read More
Top Doctors For Abdominal Hysterectomy Treatments






































































































Top Hospitals For Abdominal Hysterectomy Treatments











































Abdominal Hysterectomy
What is an Abdominal Hysterectomy
Abdominal hysterectomy, a surgical procedure first performed in 1843, involves the uterus being removed through an incision in the lower abdomen. Several other hysterectomy techniques such as the laparoscopic, vaginal, robot-assisted, or a combination of two methods have been used over the years. The approach to hysterectomy, however, depends on the indication, surgeon’s technical experience or preference, availability of resources, patient preference, and health status.
Due to the development of minimally invasive techniques, there has been a decline in the rates of abdominal hysterectomies.

Indications
- Uterine size: It has been speculated that an enlarged uterus is a common indication of abdominal hysterectomy. This is to aid in better visualization and exposure of the organ, thus decreasing the risks of severe bleeding and trauma to surrounding tissues or organs. There are no specific recommendations for which size is large enough for an abdominal hysterectomy to be performed.
- Leiomyomas: Leiomyomas, also called fibroids, are noncancerous growths of the uterine muscle. They are common in up to one-third of women and can be managed through a hysterectomy if severe or recurrent following surgical removal.
- Cancer: Cancer of the uterus (endometrium), cervix, or ovaries especially in early stages may require a hysterectomy.
- Abnormal uterine bleeding: Excessive uterine bleeding (menorrhagia) following childbirth or other uterine conditions may result in a hysterectomy following a failure of a conservative management approach.
- Pelvic organ prolapse: Prolapse of the uterus and associated structures in women can lead to a hysterectomy. This is common in women with multiple pregnancies or birth and heavy lifters.
- Endometrial hyperplasia: Endometrial hyperplasia refers to the excessive growth of the endometrium. It can sometimes lead to endometrial cancer. The conservative approach is usually preferred especially in younger women who wish to have children.
- Endometriosis and chronic pelvic pain: Most causes of chronic pelvic pain such as endometriosis can be an indication for an abdominal hysterectomy when alternative procedures are not possible or fruitful.
Contraindications
Like most surgical procedures, if the procedure is harmful, not of benefit to the patient, and is not the best alternative depending on the circumstances then it is contraindicated.
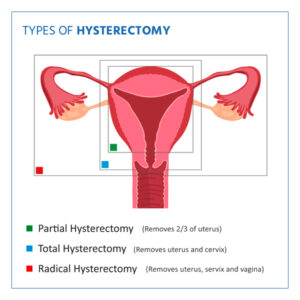
Types of Abdominal Hysterectomy
- Total hysterectomy: This involves the removal of the uterus and cervix, leaving the ovaries.
- Supracervical hysterectomy: Unlike the total hysterectomy, the uterus is removed, leaving the cervix and the ovaries. Women who undergo this procedure need to perform routine pap smears and may still experience mensuration since the cervix is attached to a section of the uterus.
- Total hysterectomy with bilateral salpingo-oophorectomy: In addition to the removal of the uterus and cervix, the fallopian tubes and ovaries are also removed (salpingectomy and oophorectomy, respectively).
- Radical hysterectomy with bilateral salpingo-oophorectomy: This involves the removal of the uterus, cervix, fallopian tubes, ovaries, the upper portion of the vagina, and some surrounding tissue and lymph nodes. This is usually indicated in cancer cases.
{kind=link}
Procedure
Standard preoperative testing may include a physical examination, EKG, chest X-ray, and blood testing, depending on the age and health status of the patient.
Abdominal hysterectomy is performed in an aseptic environment and may be done under general or spinal anesthesia. The surgical incision is made either in a midline or low transverse pattern. Blood vessels are clamped and ligated and depending on the type of necessary tissues cut. The surgical incision is then closed.
Postoperative management includes the administration of fluids, pain medications, and antibiotics.
Post-surgical Complications
-
Hemorrhage:
Research has shown that abdominal hysterectomy has the highest record of hemorrhage with as much as 400ml of blood lost during the procedure in comparison with other techniques for hysterectomy.
-
Infection:
Post-surgical infections following an abdominal hysterectomy can occur in about 10 percent of women. This is treated using appropriate antibiotics and could be due to septic surgical conditions or postoperative contamination of the surgical site. In severe cases, further surgery may be recommended. Some of the common post-surgical infections include urinary tract infections, pelvic abscesses, infected hematoma, wound infection, and vaginal cuff cellulitis.
- Constipation:
Constipation is a common side effect of hysterectomy in women and can usually be managed through the use of laxatives and an increase in dietary fiber.
- Nerve damage:
Damage to the nerve especially the femoral nerve is a common form of neuropathy in abdominal hysterectomy. Damage to the obturator nerve can also occur due to excessive stretching of the fascia or by crushing by the surgical clamps.
- Urinary retention:
Urinary retention (the inability to pass urine), can occur after an abdominal hysterectomy. However, it is more common in vaginal hysterectomy Urine can be drained using a catheter until retention resolves.
- Blood clot:
Abdominal hysterectomy, like other pelvic surgeries, increases the risk of deep venous thrombosis (DVT) and pulmonary embolism (PE) occurrence. Thus, the use of thromboprophylaxis is necessary prior to surgery.
- Damage to adjacent organs:
In addition to nerve damage, tissues, and structures, such as the urinary bladder, ureter, and urethra, may be inadvertently damaged. It is also noteworthy that the muscles, spleen, and liver could also be traumatized during the procedure.
- Early menopause:
Early menopause may occur in women who undergo a hysterectomy even with the ovaries present. This may be due to a lack of blood supply following the removal of the uterus.
- Wound dehiscence:
There may be surgical wound dehiscence in the days following the surgery. However, the most common form of dehiscence is the vaginal cuff dehiscence. This can occur within days or years after the surgical procedure. The separation of the vaginal cuff may be along the entire length or localized to a portion of the vaginal incision and can be of partial or full thickness. The evisceration of intraperitoneal fluids through tissue separation is the vaginal cuff dehiscence complication that causes the most anxiety. Total abdominal hysterectomy has been associated with a lower risk of vaginal cuff dehiscence compared to laparoscopic procedures.
Conclusion
It is important for a complete examination of potential candidates for an abdominal hysterectomy to be performed and for risk factors addressed prior to surgery. This would ensure that alternative procedures, (both conservative and surgical), would be evaluated and the best course of action taken by the physician to avoid unwanted scenarios.