Spindle Cell Lipoma
Introduction Spindle cell lipoma (SCL), first described by Enzinger and Harvey in 1975, is a benign lesion similar to a pleomorphic lipoma. It is a rare type of lipoma that contains spindle cells and grows mostly in the subcutaneous tissues, but purely dermal tumors may also occur. It is reported in about 1.5% of all… Read More
Top Doctors For Spindle Cell Lipoma Treatments
















































Top Hospitals For Spindle Cell Lipoma Treatments










































Spindle Cell Lipoma
Introduction
Spindle cell lipoma (SCL), first described by Enzinger and Harvey in 1975, is a benign lesion similar to a pleomorphic lipoma. It is a rare type of lipoma that contains spindle cells and grows mostly in the subcutaneous tissues, but purely dermal tumors may also occur. It is reported in about 1.5% of all lipomatous tumors.
Spindle cell lipoma often develops in the back, shoulder, and posterior neck. However, there have been reported cases of its occurrence at other sites albeit, rarely. They are usually well-circumscribed.
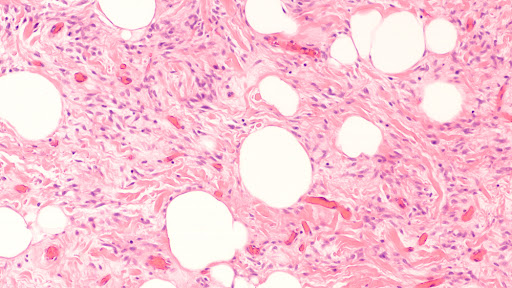
Spindle cell lipoma as their name suggests, contains bland spindle cells, a varying mixture of mature adipocytes, and ropy collagen fibers. Histologically, there are two variants:
- The classical spindle cell lipoma which contains adipose tissues with scant spindle cell areas and
- The fat-free variant with more spindle cells and very few fatty tissues.
Predisposition and Causes of Spindle Cell Lipoma
Most spindle cell lipomas occur in adults between the ages of 40 and 60. Although men between the ages of 45 to 70 are more affected. The incidence in men and individuals assigned as male at birth is higher than in women and individuals assigned female at birth (less than 10% of cases occur in women). In people 20 years and below, the condition is rarely recorded.
Research also suggests that genetic mutations in individuals and possible inheritance for biological parents may predispose an individual to the occurrence of spindle cell lipoma.
Clinical Signs and Symptoms
- It usually occurs as a lump under the skin.
- May be slightly movable on palpation.
- It is usually painless.
Diagnosis of Spindle Cell Lipoma
Diagnosis of spindle cell lipoma is done through blood work, cytology, histology, and cytogenetics. It is also important to consider the clinical signs on presentation to the hospital.
Cytology is done via fine needle aspiration. The results may be as characteristic of histology.
However, with tumors in atypical locations, even aspirates containing all of the characteristic elements may be difficult to use for a firm diagnosis of SCL.
Radiographic imaging e.g. MRI or CT scan, could also serve as a means of diagnosis, especially in cases where a sarcoma is suspected.
Differential Diagnosis of Spindle Cell Lipoma
- Pleomorphic lipoma: Pleomorphic lipoma and spindle cell lipoma are currently regarded as morphologic variants of a single neoplasm. The lesions are the same cytogenetically as spindle cell lipoma.
- Solitary fibrous tumor: These have bland spindle cells that resemble spindle cell lipomas and ropey collagen, and they are CD34 positive. The absence of adipose tissues within the solitary fibrous tumor is helpful but may be difficult to differentiate from fat-free SCL.
- Spindle cell tumors such as liposarcoma, schwannoma, neurofibroma, angiolipoma, dermatofibrosarcoma protuberans, etc.
- Myxoid lesions e.g. myxoid neurofibroma, myxoma, myxoid fibrosarcoma, myxoid liposarcoma, etc.
- Epidermoid cyst: In contrast to SCL, this is usually an accumulation of skin cells, fluid, pus, etc.
- Sarcoidosis: This contains granulomatous growths arising from the clumping of inflammatory cells.
- Subcutaneous tumors e.g. basal cell carcinoma, melanoma, and squamous cell carcinoma.
- Nodular fasciitis
- Weber-Christian panniculitis
- Erythema nodosum
- Nodular subcutaneous fat necrosis
- Vasculitic nodules: This is an inflammation of vessels that occur in response to diseases like tuberculosis or reaction to some drugs.
- Rheumatoid nodules: This is an inflammation-induced swelling and occurs over joints.
- Infections (e.g. onchocerciasis, loiasis)
- Haematoma: A hematoma occurs when a blood clot forms in an organ, tissue, or body space following a rupture of a blood vessel.
Management of Spindle Cell Lipoma
Spindle cell lipomas are usually harmless and as such, no medical intervention may be needed. In some instances, the growth may cause discomfort in daily activities or may not be desired for aesthetic reasons.
Treatment may be non-surgical or surgical depending on the size, location, age, health status, and preference of the health practitioner. Non-excisional treatment of lipomas includes the use of steroid injections and liposuction which are more commonplace than the surgical approach.
Steroid injections into the tissues aim to cause local fat atrophy. This causes the lipoma to shrink and in very rare cases, eliminate the lesion. This is best done with SCL of less than 1-inch diameter. Lidocaine and triamcinolone acetonide are mixed in a ratio of one to one and injected into the center of the mass. This may be repeated several times every month for better effect. The major complications arise from the injections and can be minimized through a reduction in volume and proper needle placement.
Liposuction can be used to remove both small and large SCL especially if it is located in an area where large scars should be avoided. This can be done with a 16-gauge needle and has fewer complications than large cannula liposuction.
Surgical management involves the excision of the SCL under local or general anesthesia. Surgical excision usually ensures total removal of the lipoma, unlike the other non-surgical methods of management. The patient is put under anesthesia for the procedure. The main surgery involves either an enucleation or an excision.
- Enucleation: This is used for small lipomas. Over the lipoma, a 3 to 4-mm incision is made. Using a curette, the lipoma is freed from surrounding tissues and removed from the incision wound. No stitches are usually required rather a pressure dressing is applied to prevent hematoma formation.
- Excision: For larger lipomas, a longer incision is made over the overlying skin and blunt dissection of the lipoma is done. It is necessary to be careful as the lipoma is sometimes highly vascularized. A stitch is used to close the incision line.

{kind=link}
Complications of Lipoma Excision
The possible complications associated with the surgical management of a spindle cell lipoma include:
- Post-surgical infection especially when the procedure was done in septic conditions.
- Ecchymosis due to trauma.
- Injury to nearby nerves due to physical damage or anesthesia.
- Injury to nearby blood vessels and possible hematoma formation.
- Permanent deformity secondary to removal of a large lesion
- Excessive scarring with cosmetic deformity or contracture
- Injury to surrounding muscle
- Fat embolus
- Periostitis/osteomyelitis
- Seroma
In conclusion, spindle cell lipoma is usually a non-life-threatening condition and thus, no medical intervention is required except for aesthetic reasons or when it is growing, painful, tender, or warm to touch and interfering with regular day-to-day activities.